Introduction
A cluster of pneumonia cases of unknown aetiology was reported to the World Health Organization (WHO) from the Wuhan city, Hubei province of China on the 31st of December, 2019. The organism was identified as a novel form of Coronavirus on 7th January 2020 and named as 2019-nCoV. This took the form of a pandemic and was declared Public Health Emergency of International Concern (PHEIC) by 30th January 2020. The disease was later re-named as Corona Virus Disease 2019 (COVID-19).1, 2 As on 25th March 2020 midnight, around 198 countries and one international conveyance have been affected. The disease entered into Phase VI pandemic within 2 months with highest ever reported number of cases and deaths by any pandemic of the modern era (4,79,840 cases, 21,576 deaths and case fatality rate 4.5%).3
As the outbreak of corona virus disease 2019 (COVID-19) is rapidly expanding in India and beyond, with the potential to become a worldwide pandemic,1 real-time analyses of epidemiological data are needed to increase situational awareness and inform interventions.2 The real-time analyses have shed light on the transmissibility, severity and natural history of an emerging pathogen in the first few weeks of an outbreak, such as with severe acute respiratory syndrome (SARS), the 2009 influenza pandemic, and Ebola.3, 4, 5, 6 Analyses of detailed line lists of patients are particularly useful to infer key epidemiological parameters, such as the incubation and infectious periods, and delays between infection and detection, isolation, and reporting of cases.3, 4
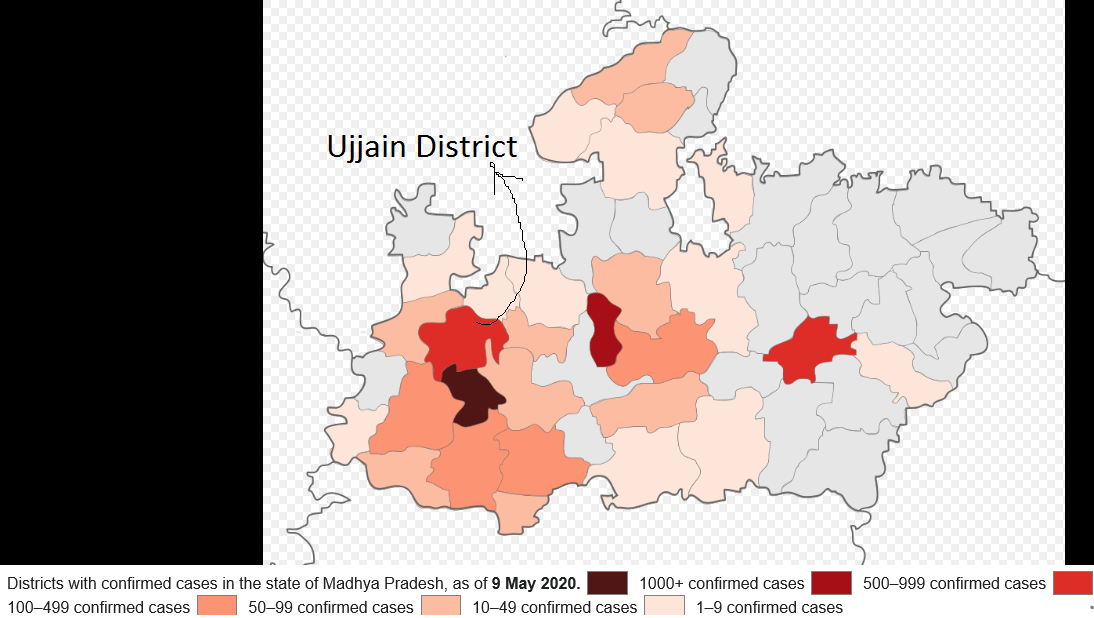
The first case of the COVID-19 pandemic in India was reported on 30 January 2020 and The first cases of the COVID-19 pandemic in Madhya Pradesh (Figure 1) were confirmed on 20 March 2020.7 These were the first four cases in Jabalpur, Madhya Pradesh. The state has confirmed a total of 7,024 cases, including 305 deaths and 3,689 recoveries, as of 26 May 2020. In Ujjain district first case appears on March 22 and till 23 May, number of cases reached to a total of 235 cases with 45 deaths. The death fatality rate of the district is well above the national death rate of 2.87 with 19.14.
The objective of the study was to find out epidemiological linkage among corona cases in the town and various action/measures done by local health/administration. This study was done to explore the reasons of positivity in a small town with high death rate.
Methodology
About the town
A cluster of Covid and non Covid confirmed death cases of a big family in a small town Badnagar, District Ujjain, Madhy Pradesh was recorded in March end and first two weeks of April 2020. Till 23rd May 2020 the town has 74 positive cases. The rate of positivity in response of samples taken is 17.4%. All the cases have only background of two index cases in the town. This epidemiological study revels that out of two the one index case in the town is becomes an ideal example of local transmission of Corona disease spread and another index case is becomes another example of proper measures and follow up of guidelines can break the chain of transmission. In an epidemic or pandemic of contagious disease society must follow the rules, guidelines, lockdowns which normally does not suits to the common people. In initial stage besides all the measures taken by the government, common people take it very lightly and the consequences are profoundly serious.

Badnagar is a Municipality town in district of Ujjain, Madhya Pradesh (Figure 2). The Badnagar town is divided into 20 wards and have estimated population of 48,000. In the Municipality, Female Sex Ratio is of 945 against state average of 931. Moreover, Child Sex Ratio in Badnagar is around 896 compared to Madhya Pradesh state average of 918. Literacy rate of Badnagar town is 83.89% higher than state average of 69.32%. Male literacy is around 90.14% while female literacy rate is 77.32%. The religion wise data revels that out of total town population is distributed as 66.72% Hindu, 26.72% Muslim, 5.88% Jain and rest distributed in the Christen, Sikh and other religions. The town is known for its old heritage and big joint families. The town is very dense just like other old cities in Madhya Pradesh. The social fabric of the town is traditional and social unlike the metros and big cities. The western culture affects the town but people are so cultural and person to person bonding is high. More or less most of the people are comparatively relaxed and with less stress. The town covers above 300 villages and prosperous in nature. Literacy rate of the town reveals the high education level. Most of the families have business or agriculture and allied activities. In the town private and government job dependants are comparatively less in nature.
Initiation
This study was conducted in one month duration started with Letter from Regional Joint Director, Ujjain Division, Ujjain with approval Dean Government Medical College, Ratlam.
Study design
The study was descriptive in nature. An exloratory analysis was done for all cases of COVID-19 diagnosed in town as of the end of May 23, 2020. A public health emergency was declared, and a formal investigation began from March 25 to 23 May 2020. Although individual informed consent was not required for this study, all data were handled as a deidentified set to protect patient privacy and confidentiality.
Visit plan
Day 1- The team visited to the facility on 20 may and meet with I/c Medical officer, Nodal COVID-19 Officer and review the status of situation. All the details of COVID-19 till date was reviewed and also the details of process followed till date was assessed. Later on team met with Sub Divisional Magistrate (SDO) and Chief Municipal Officer of the city to assess administrative points followed till date.
Day 2 - Met with I/c RRT, RRT Team Members and Survey team to assess the contact tracing, contentment area survey and survey non-affected area.
Day 3 - Met with IDSP (Integrated Disease Surveillance Programme) cell and collect all necessary information to review the process.
Day 4 - Team visited to the contentment area and assess the guidelines followed for making an containment areas and measures taken at perimeter control. Team also reviewed the sampling process in form of PPE measures, Process of sampling and packaging of sample. Team visited to recently opened containment areas and met with cured positive patients. Team also meet with families of suspected Index case and gathered the necessary information to identify the cause of infection and Index case.
Data source
By categorizing COVID-19 as a notifiable disease, as per guidelines all cases to be immediately reported to Integrated Disease Surveillance System (IDSP). Entry of each case into the system was performed by local epidemiologists and public health workers who investigated and collected information on possible exposures. All cases were recorded in proper IDSP format. All case records contain in particular IDSP formats, all cases have records in the system and no records are duplicated. No sampling was done to achieve a predetermined study size and no eligibility criteria were used and all cases were included.
Variables
Patient characteristics were collected at baseline, meaning the time of diagnosis, epidemiological investigation, symptoms, without symptoms only based on contact with positive person. Patients were categorized as age, sex, morbidity condition. The contact history was collected and to identify the index case/s. Linkages between the cases, if any. For construction of epidemiological curves, date of onset was defined as the date on which patients self-reported the start of either fever or cough during epidemiological investigation. Cases were categorized as confirmed, suspected, clinically diagnosed or asymptomatic.
Results & Observations
The sequence of events
The cases were arising when the whole country was under lockdown and starting phase of Coronavirus spread in the Ujjain District. Madhya Pradesh recorded its first death of positive case of COVID on 22 March. A woman aged 65 years with co morbid condition like diabetes. She was critical and had serious pulmonary complications. In the town Badnagar a businessman aged 42 visited nearby Indore city for business purpose for three to four days. On March 30 his father aged 66 years sudden collapse and died at home. He also has cardiac problem since three-four years and died due to sudden cardiac arrest so he was not taken as suspected for Covid. He was a part of 130-member family living in different clusters in the town. On his death family members assemble for next few days for rituals. In the continuation of this on 8 April the businessmen son was died who travelled the nearby city. He got Influenza like illness on 27 March before his father’s death. He had a regular practice to take alcohol and suffered with Alcoholic liver disease and a week before he was also taking treatment for typhoid. Naturally, his immune system was very low. On his death 4 samples were taken on 8 April of his family and on 19 April reports were found negative. The sampling was done by the district level team and there was no facility at town civil hospital at that time.
On 19 April a vegetable hole sale dealer came with symptoms of corona with travel history and contact with positive persons. Person immediately referred to district level stipulated covid care hospital and his report found positive. Samples of contacts were also sent.

On 20 April, two deaths occurred again in big family in morning and afternoon. One dead body with three of his family member's sample was taken on same day. All of them found positive on 23rd April. On 23rd April 22 more samples were taken with contact history including one female member who was died on same day. On 27th April total 6 people found positive, it includes the female who died. From second family his two more members were found positive on same day. (Tree showing index case 1 and their contacts)
On 24 April 26 more samples were taken from big family, and they all put in quarantine at government designated facility. Report of 6 positive and 4 suspected positive received on 29 April. In total, that big family had 16 postive cases till now, rest positive cases from other families.
A person from big family who was died and positive in a nursing home of the town, contact tracing of that nursing home was done on 25 April and sent 11 samples. Among 11 four were found positive on 29 April. Again, the contact tracing was done and on 26 to 28th April total 25 samples were sent. In all local transmission of disease happened in the town and up to 23rd May four new families got infected.
In contact tracing of nursing home and big family, other four families were found infected and from these families, it was spreading to near by area. Total around 5000 population was under 7 containment zone. Total 3 corona positive deaths and total of 74 positive cases were recorded up to 23 May.
Figure 4
Index cases 1 and 2 in Badnagar and local transmission of cases to seven families (Red dots on the tree are showing the positive cases)
Family 1$: Family of Index case (Total Case- 32)
Family 2@: Family of Neighbour (Total Case- 6)
Family 3*: Treating physician family (Total Case- 11)
Family 4#: Family of Patient admitted adjacent bed of index case (Total Case- 2)
Family 5**: Family residing in first containment area (Total Case- 11)
Family 6##: Family residing nearby containment area (Total case- 9)

Containment area
A total of 15 containment areas were formed in this town. Four active containment areas were there on the day of visit. The areas were small in size. The small sized containment areas were made due to administrative reasons but the health point of view it may be risky. Team observed that the monitoring of the containment areas was poor. The surveillance system through CCTV etc. was not proper and public monitoring was lethargic. The disease was mostly spread in old Badnagar areas and old town have very narrow roads and congested housing.


Sampling process
The team also monitor the sampling process. As per guidelines paramedical taking samples in proper manner but doffing was not aligning with the rules. The samples were collected by two trained lab technicians and sent to district level administration. Sample sending process should be streamline and for better efficient testing, sample must be sent directly to testing facility. Total 455 samples collected- result received-449- 6 rejected- positive-74-negative – 375.
Facility audit
In the town only two quarantine facilities are available and there is no CCC (Covid Care Centre) facility. The quarantine facility was not proper gurded. The town have 3 RRT (Rapid Response Team) facility but these were deployed very late.
Contact tracing and screening
Total contact tracing of 432 people done in the town against 74 positive cases. Average 6 people per positive. As the team finds that most of the cases came from these contact tracing. It reflects the local transmission of virus from the Index cases. No other transmission link available in the town.
Data collection and interpretation
In Badnagar town the first case found positive on 23 April and up to 23 May total 455 samples were taken and sent for testing on authorized centers. The trend of samples sent is given Figure 7.

In the initial stage the samples were taken by the district team, so frequencies of samples are slow or no samples taken. As the local transmission increased, the screening increase and sampling process were also increased.
Age wise distribution of 74 positive patients shown in Figure 8 and it revealed that most vulnerable group was young generation aged between 18 to 40 years. Because they had maximum mobility and activity to go out outside for complition of family related tasks. The sex-wise distribution shows (Figure 8) the equality in cases. It also reflects that all the positive cases are coming from total six families so it gives direction that the transmission may be spread through families. In the process of the study, general local interview with the positive patient’s families found that in the initial stage a death occurred in big family and as a part of ritual all the 130 members were regularly visited for 13 days to the pay homage and may get infection.
Three positive deaths happened during the study period of March 25 to 23 May 2020. There were three deaths during study period. All of them were above 60 years of age (2 males and one female). These three people have severe co morbidity like heart and spine relates issues. The difference in number of days between sample taken and report received was surprisingly not in order. As Figure 10 reflects that, about 66% samples received reports after 10 days or more.



In starting the delay in reporting was huge and as facilities develop for the samples testing the delay reduces to one day. But still delay in report receiving is major technical issue which may cause the damage.

In Figure 11 date-wise positive cases were represented and it didnot show any trend because there is prfound delay in sample collection and reporting.
Discussion
In the present study on the basis of data and discussion on ground, finds two index cases in the Badnagar Town which makes a chain of local transmission and reached up to 74 positive people. Initially there was no facility at civil hospital to take the samples and team came from district level. The mechanism of samples was too complicated and in this regard the efficacy was compromised. As we see in Figure 9 that around 66% samples got result after more than ten days. Guidelines for the management of corona suspected cases and rules for samples were not clear in initial stage and result of these first three deaths in the town were un-noticed. From the study the first index case may be start from this stage and movement was happened due to these deaths create proper atmosphere for local spread. Figure 9 reveals that male and female contributes equal in positivity and only six families affected by the positive case, it implies the family to family local transmission of the virus.
The second index case was a vegetable wholesale dealer. He came by himself to the facility with corona like symptoms and commits the movement in nearby areas. He sent to the district for further management. He found positive on 19 April and his residence area was put under containment, his family was put under quarantine. Immediate action and prompt response stop the further transmission of virus. Although, his wife was found positive but no further case increases in the area. It is evident from contact tracing that in the town after lockdown private clinics were running and caused a new chain of positivity.
The test positivity rate and death rate are 16.22 and 4.02 respectively, which are very high in compared to both state and national level.
Conclusion
The Badnagar town suffered with corona positivity with a great extant through mainly local transmission with two index cases. Range of patients were 5 months to 68 years and almost equally distributes among male and female. Big families, narrow roads, congested housing and “Otla culture” (People sit in the evening to pass the time with some games or simple talking), not maintaining the proper social distance, follow the death rituals with the whole family, not maintaining lockdown guidelines were the public point of view resigns for spreading the disease. From administrative point of view small-small containment area, no proper guarding and surveillance of the areas, Private clinics were open besides the strict guidelines, quarantine centers must be guarded were the major reasons for stimulating the situation. From health point of view the management of sample taken and process of sending was poor in initial stages, it was letter much better, but damage was done. Almost 66% of the samples got result after more than 10 days of delay. For doffing and donning of PPE kits must be given training to peramedicals from time to time and RRT team came into the picture very late were the main reasons of high rate of test positivity rate and death rate 16.22 and 4.02 respectively.
Recommendations
If mistakes are happened, it means work is done with full capacity, but directions and management is required for optimum and best results. Every pressure and challenging situation give best out of the system. This was what happened in Badnagar town. Some recommendations suggested after completing the research are as follows-
Proper and clear-cut guidelines from higher authorities makes the path extremely easy.
Sample management must be improved i.e. samples directly sent to testing faculties. It will reduce the time and in time reached for testing.
Donning and doffing of PPE must be repeated to the paramedical to guard themselves and other health personnel.
Containment area and quarantine facility may be properly guarded through electronically like Drone, CCTV etc. and by policing.
The containment area may be decided not only on administrative basis but also health point of view. It requires health and administrative official’s coordination.
Town requires CCC (Covid Care Centre) facility, as some of the Government buildings & Nursing homes are available for the purpose.
RRT is core team to deal with any epidemic. RRT must be deployed from the beginning of epidemic.
In depth IEC to ensure the massage of intensity of contagious disease may be given through mikeing etc. for increasing awareness among people. The massage mayn’t be given in order form but at humanitarian ground, as everybody is in lockdown and feeling anxiety and fear.
The most effective strategy to control this pandemic disease during all stages of transmission is source reduction. Universal use of face mask, hand hygiene (washing through soap and water) and cough etiquette should be adopted by all with specially by high risk population.
Physical distancing norms need to be practiced slowing down the spread of infection. At the same time, enhanced social bonding measures need to be promoted to address mental health concerns of anxiety and lockdown. Stigma and discrimination in COVID-19 tend to be associated with specific population groups (such as religious groups or returnee migrants) even though not everyone in those groups is specifically at risk. Stigma can also occur after a person has been released from COVID-19 quarantine.
Governments, media and local organizations need to be pro-active by making people aware and treating them with empathy and respect.
There should be constitute a panel inter disciplinary experts under administrative head, health staff should give technical inputs to control the disease.
It is important to conduct extensive surveillance for Influenza like Illnesses (ILI) through ASHA/ANMs/MPWs, and Severe Acute Respiratory Illness (SARI) through clinical institutions (including private hospitals), daily reporting to identify geographic and temporal clustering of cases to trace transmission foci (hot spots / cluster events). This must be supported by trained epidemiologists from nearby medical colleges (Govt. Medical College, Ratlam or RD Gardi Medical College, Ujjain) and public health institutions.
Field survey team may be equipped with some Medicine like (Vitamin B complex or Vitamin C, ORS) or Ayurvedic Kadha. Which can be distributed to public. This will improve the feedback quality.
Only two technicians were training in Block for Covid sampling. So as per current and upcoming scenario, human resource facility needs a rigorous review and planning. This also required a continuous training of existing staff for upcoming revised guidelines.