- Visibility 306 Views
- Downloads 11 Downloads
- DOI 10.18231/j.ijfcm.2022.007
-
CrossMark

Pneumothorax — A rare cause of delayed death in hanging
Introduction
The suicidal rate in India during 2020 is 11.3 per lakh population as per NCBR statistics 2020.[1] Among the various methods of committing suicide, the incidence of hanging is approximately 57.8% of total cases of suicide as per NCBR statistics 2020.[1] In the cases of hanging, the usual fatal period is 3 to 5 min.[2] Death is usually due to asphyxia or venous congestion or cerebral anemia or reflex vagal inhibition leading to cardiac arrest or injury to the cervical vertebrae.[2] Here, we report a rare case of hanging in which the victim survived for three days after hanging and succumbed to one or more delayed complications as mentioned in the hospital records — Left Pneumothorax/ pneumomediastinum/ Subcutaneous Emphysema/ Aspiration Pneumonitis / Hypoxic Ischaemic Encephalopathy/ Brain Stem Dysfunction and Sepsis.
Case history
A 24-year-old, married, female was brought to the emergency room in an intubated state with alleged history of hanging in her residence. On further questioning, her husband gave history that attenders found herself hanged by a saree to a ceiling fan with both feet touching the ground (last seen was 20 minutes before the incident). She was rescued and brought to nearby hospital where she was intubated due to poor GCS and referred to our tertiary care center.
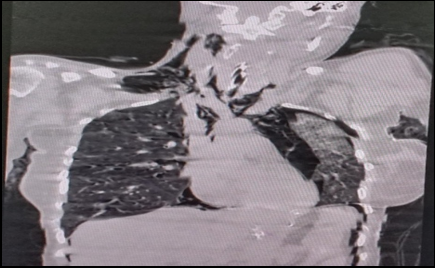
During admission, vitals were maintained with ACMV — endotracheal mechanical ventilation. SPO2 -91%, Blood Pressure -120/80 mm of Hg, Pulse Rate -120/min. The initial cranio cervical thoracic computed tomography on the day 1 of incident showed normal study of brain and cervical bones, left pneumothorax, pneumomediastinum with extension of sub cutaneous emphysema on right side of neck, collapsed left lung and left lower lobe consolidation ([Figure 1]). She was treated with intravenous fluids, diuretics, steroids, antibiotics and antiepileptic drugs. Inter Costal Drainage tube was inserted on the left hemithorax as per guidelines for management of pneumothorax. The patient’s condition deteriorated on the day 2 of admission. She was supported with noradrenaline infusion. In spite of all above measures, she expired on Day 3 of admission. Body was sent to mortuary.
After receiving request for post mortem examination from the Investigating Officer, Autopsy was done. The following findings were noted in autopsy — Moderately nourished and moderately built female body with bluish discoloration of gums and nail bed of all the fingers and toes; post-mortem hypo stasis fixed on the back with areas of contact pallor; cornea — hazy; pupils — dilated and fixed; height- 160 cm.
Irregular healed abrasions with reddish brown scab firmly adherent to the base: a) 0.5 x 0.5 cm on the back of right elbow; b) 1 x 0.5 cm on the front of middle third of left leg.
A well - defined, incomplete, asymmetrically oblique reddish brown ligature abrasion ([Figure 2]): 23 x 3 – 0.5 cm on the front and sides of the neck, with intervening area of normal skin for 3 cm to the right of midline, above the level of thyroid cartilage; on the front of neck, the ligature abrasion was 4 cm below the chin and 9 cm above the suprasternal notch; on the right side of neck it was at the level of angle of right side of mandible and on the left side of neck it was 7 cm below the left Mastoid process; it was merged with hairline on the left side of back of neck; on dissection of neck: Base of the ligature abrasion was dry, pale and parchment like; Larynx and Trachea: Empty and intact; Dark red bruising 3 x 1 x 1 cm of the middle third of sternomastoid muscle on the right side of neck; Hyoid bone and other laryngeal cartilaginous structures, soft tissues and the Major Blood vessels of neck were intact.
Surgical incised wound 2 x 1 cm x cavity deep on the lower and outer aspect of left side of chest — Intercostal Drainage Tube wound ([Figure 3]).
No other external or internal injuries anywhere on the body
Heart: Normal in size; multiple sub-epicardial petechial haemorrhages on both the surface of heart; cut section: All Chambers contained fluid and clotted blood; Valves: Normal; Both the Coronary Ostia: Patent; Coronaries and Great vessels: Normal.
Lungs: Normal in size; multiple sub-pleural petechial haemorrhages on the surface and interlobar fissure of both the lungs; firm in consistency; cut section: Frothy fluid oozed out from the congested cut surface.
Stomach: Contained 200 grams of partly digested food particles with no definite smell; mucosa: Patchy areas of congestion.
Liver, Pancreas, Spleen and Kidneys: Normal in size; cut section: Congested.
Bladder: Empty and intact.
Uterus: Empty and intact.
Scalp, Vault, Duramater and Base of Skull: Intact; Brain: Soft and oedematous; surface vessels: Congested. cut section: Normal. Ribs, Pelvis and Spinal column: Intact. Viscera preserved and sent for chemical analysis.
Tissue bits preserved for Histopathological examination.


Opinion as to the cause of Death — Reserved pending the reports of chemical analysis of viscera and Histopathological examination of Tissue bits.
Viscera report came as negative for Alcohol and/or Poison
HPE report
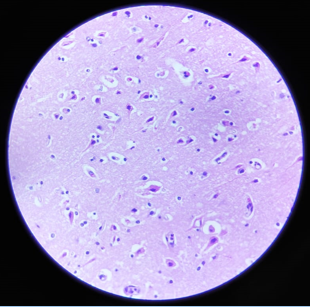
Brain and Brainstem–Features of hypoxic ischemic encephalopathy. ([Figure 4])
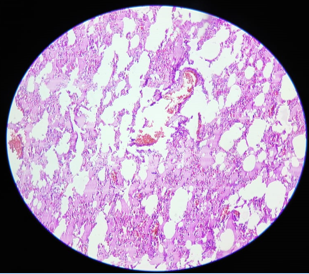
Lung — Features of pulmonary edema and haemorrhage. ([Figure 5])
Liver — Normal histology.
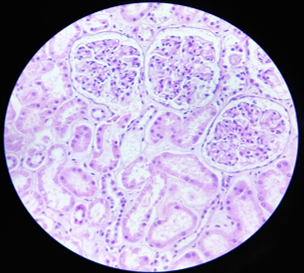
Kidney — Features of acute tubular necrosis and foci of haemorrhage. ([Figure 6])
After obtaining the reports of chemical analysis of viscera and Histopathological examination of tissue bits, Opinion as to the cause of Death was given as the deceased would appear to have died due to the effects of Hanging.
Discussion
Among the various methods of committing suicide, Hanging is a common method as per NCBR statistics 2020.[1] Hanging (SELF SUSPENSION) is a form of asphyxia that is caused by the suspension of the body by a ligature encircling the neck, where the constricting force being the weight of the body.[2] The term “near hanging” refers to a patient who survives a hanging injury long enough to reach the hospital.[3] In the near hanging cases, the delayed fatality occurs due to aspiration pneumonia, infections, edema of lungs and larynx, hypoxic encephalopathy, infarction and abscess of the brain, cerebral softening.[2], [3] Most of the patients develop respiratory and neurological complications immediately after the rescue. In our case, it is complicated — associated with pneumothorax.[4]
The respiration against the obstructed airway in hanging, causes increased intrathoracic pressure leading to rupture of pulmonary alveoli. The air escapes along the bronchi to the connective tissue of the mediastinum and neck and also to the thoracic cavity.[5], [6] This Macklin effect also explains why pneumomediastinum can develop after blunt thoracic trauma and with positive pressure mechanical ventilation.[6] In our case, the development of pneumomediastinum and pneumothorax is either due to resuscitation and mechanical ventilation or the process of hanging itself.
In our case, the hanging patient presented with pneumothorax/ pneumomediastinum/ Subcutaneous Emphysema and succumbed to death after three days of admission due to pneumothorax/ pneumomediastinum/ Subcutaneous Emphysema / Aspiration Pneumonitis / Hypoxic Ischaemic Encephalopathy/ and Sepsis.
Picetti E et al described a similar case of a hanging in which the patient developed pneumomediastinum and subcutaneous emphysema of the neck who eventually recovered fully after the treatment.[5]
Thabouillot O et al. reported a case of hanging with pneumothorax and pneumomediastinum in which the patient died from multi-organ dysfunction syndrome (MODS) after 48 hours of admission.[7]
Conclusion
Death in hanging is almost immediate. Death in near-hanging victims-Delayed death is rare. The presence of pneumothorax is rare in rarity.
Though it is rare, the presence of pneumothorax and pneumomediastinum has to be ruled out in all cases of hanging before starting on mechanical ventilation or immediately after starting on mechanical ventilation to safe guard us from the future allegation of iatrogenic barotrauma subsequent to mechanical ventilation and also to prevent further aggravation of existing pneumo thorax and pneumo mediastinum. Any hemodynamic deterioration in a case of attempted hanging patients, the presence of pneumothorax has to be thought and ruled out.
Post-mortem radiological investigations in all cases of hanging, may reveal more cases of pneumothorax/ pneumomediastinum/Subcutaneous Emphysema.
Source of Funding
None.
Conflict of Interest
None.
References
- . Accidental Deaths & Suicides in India-2020. 2022. [Google Scholar]
- K S N Reddy. The essentials of forensic medicine & toxicology. 2017. [Google Scholar]
- A Kumar. A Case Report on Delayed Death in Attempted Hanging. Int J Curr Adv Res 2018. [Google Scholar] [Crossref]
- M D Nithin, B Manjulatha, P Kumar, G N Sameer. Delayed death in hanging. J Forensic Res S 2011. [Google Scholar]
- E Picetti, I Rossi, V Antonini, A Volpi. Pneumomediastinum and emphysema of the neck after a suicide attempt by hanging. Minerva Anestesiol 2012. [Google Scholar]
- S Murayama, S Gibo. Spontaneous pneumomediastinum and Macklin effect: Overview and appearance on computed tomography. World J Radiol 2014. [Google Scholar] [Crossref]
- O Thabouillot, C Derkenne, K Bertho, M Huck, B Prunet. Hemodynamic Failure in a Hanging Man: Think About the Tension Pneumothorax!. Prehospital Disaster Med 2019. [Google Scholar] [Crossref]